

This post is also available in:
Imagine a health and social care service where people can use substances considered illicit – such as crack and heroin – without being judged or punished. A service where these people are welcomed and receive necessary care, rather than being on the streets, parks and alleys. In the last 20 years such services have been an integral part of the strategies for reducing theharms of drug use in a number of western European countries, North America and Australia. This blog provides a summary about these drug consumption rooms (DCRs) - what they are, their benefits, where they are possible, and what the main existing DCR models are there.

Definition and names
"DCRs are facilities where (homeless) people who are dependent on drugs can use their substances in a calmer, safer, hygienic environment, and without judgement or punishment. DCRs aim to reduce the harms to health and society related to drug use"
They offera place where people bring their illicit drugs touse; drugs are not provided.
DCRs can be known by several names, such as:
- Drug Consumption Rooms ;
- SupervisedInjectionRooms
- Supervisedconsumption Rooms
- Injection rooms
Benefits
DCRs save lives and promote access to health for people who use drugs. They also bring benefits to society in general as they assist in the prevention of communicable diseases and in reducing crime associated with use in public spaces.
Several studies prove the benefits of drug consumption rooms. In 2018 we reviewed the literature on the benefits of DCRs, specifically for people who use stimulant drugs such as crack. What we found was that the rooms help to:
- Preven t overdose
- Prevent communicable diseases
- Prevent stigma and violence associated with drug use in public spaces
- Prevent feelings of insecurity associated withuse inpublicspaces
- Promote access to health and socialservices
- Promote access to sterile and safer materials for drug use
- To prevent the loneliness and isolation of people who use drugs
Usuário da sala 1A sala de consumo pra mim é como um café, um lugar para encontrar as pessoas e conversar.
Usuário da sala 2A maneira principal em que a sala de consumo contribuiu para a minha qualidade de vida é através da alimentação. Há quase sempre alimentos saudáveis e em abundância aqui. […] Socialmente o lugar também é de grande valor. Eles são pessoas de confiança para trocar ideias, mas podem também ser um espelho para mim. Podem verificar minha saúde e dizer-me quando eu não pareço estar muito bem. Nem sempre eu consigo fazer isso sozinho.
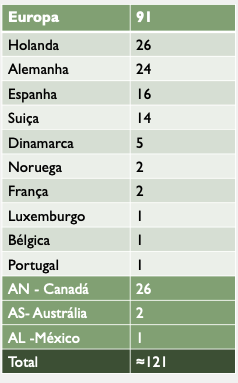
DCRs in the world
Models of DCRs
-
Integrated rooms
Integrated rooms
The integrated rooms have a number of otherassociated services to the space for drug consumption. These services can be:
- Drop-in centers
- medical and health care consultations
- mental health care
- social care
- Antagonist Opioid Therapy (such as methadone or buprenorphine for heroin users)
- income generation activities
- administrativeand legal support
- shower and clean clothes
- food
- possibility to use a phone or computer (to talk to family, arrange social or legal service issues, look for a job or make a resume, for example)
- recreationalactivities
- reference to other services
In addition to these services, users receive materials for safer drug use and information on harm reduction. The video below is an example of these type of DCRs. The first and only room in Latin America at the moment (2020), located in Mexico. The room still faces difficulties to have government support, due to prejudice against drug use. The same type of room exists and has support from government and international institutions in several other countries in Europe and North America.
2. Specialized rooms

3. Mobile rooms

4. Residential rooms

Styles and rules
DCRs can have several styles, from the most formal to the most informal.
Formal rooms have stricter rules, more hygiene and safety protocols, greater separation between users, and generally include health workers as nurses to supervise drug use. In these rooms, for example, one can have control through cameras and mirrors (as we see in the photo below), metal detectors at the entrance door, and check-ups to check if the user is bringing their own drugs. This photo room is in Canada.


How do DCRs work?
In general, people who use drugs bring their substances and have a set time to make use. This time, around 30 minutes, can be extended if there is no one waiting to use.
Users of the service are usually registered. There may be different admission criteria, for example, age-related, history of substance dependence, or being homeless. Commonly, registration is done on first access, where users also need to sign a contract agreeing to house rules.
The rules vary greatly depending on the model and style of the room and depending on the needs and preferences of service users. A good practice of several DCRs is to define the rules together with users. Fairly common rules are not to be aggressive (verbally or physically), bring your own drugs, do not sell drugs inside the DCR, and respect other users.
With regard to workers, these can be nurses, psychologists, social workers, peers, social educators, and harm reducers in general. The important thing is that workers are welcoming, create a healthy atmosphere, and contribute to improving the quality of life of the service-using population. For this, it is necessary to seek a balance between necessary safety and hygiene conditions (both for users and workers) and the needs and preferences of service users.
Substance use rooms in Brazil
Unfortunately, there are still no DCRs in Brazil. Such rooms, in the various models described here, would be extremely beneficial to welcome people who use drugs and are in a situation of vulnerability. Consumption rooms would allow these people not to have to make use of the street, exposed to police violence, community prejudice, and unhygienic conditions. It would also offer a protected space where access to other health and care services is facilitated. Such services already exist in several other countries, and their effectiveness is proven. It is a matter of political will, and pressure from organized civil society.
Which consumption room would you like to see in your city? Here are a few points to think and discuss:
- What would be the objectives ofthe service – for what and for whom it would exist?
- Which model would work better? Integrated, specialized, mobile,residential, or even a new one to be created?
- And which stile - formal or informal? What kind ofrules would be necessary?
Want to share your ideas? Write it down!
To learn more
- of Gee, A.; van der Gouwe, D.; Woods, S.; Charvet, C.; van der Poel, A. (2018) Drug Consumption Rooms in the Netherlands.
- International Network of Drug Consumption Rooms (website)
- Peacey, J. (2014) Drug Consumption Rooms in Europe. Client experience survey in Amsterdam and Rotterdam.
- Rigoni, R., Breeksema, J., Woods, S. (2019) Speed Limits. Harm Reduction for people who use stimulants. Escola Livre de Redução de Danos, Recife. (Chapter on DCRs in the Netherlands).
- Schäffer, D.; Stöver, H. (2014). Drug consumption rooms in Europe Models, best practice and challenges.
- The Global State of Harm Reduction 2020.
